



The context

"Twenty years ago, Edmond Kaiser - aware of, and appalled by the magnitude of the plight of child martyrs of noma, whom nobody seemed to care about - started insistently harassing international organizations, including WHO, and the government authorities concerned. His repeated appeals, together with Sentinelles' missions to Mali (1988), to Burkina Faso and to Niger (1992), were instrumental in launching the fight against noma, carrying out vital activity to help the young victims of this dreaded evil, which devours beauty and life." Sentinelles
Epidemiological monitoring
No reliable statistics are available on the number of cases, given the poorly developed health systems in countries where noma occurs.

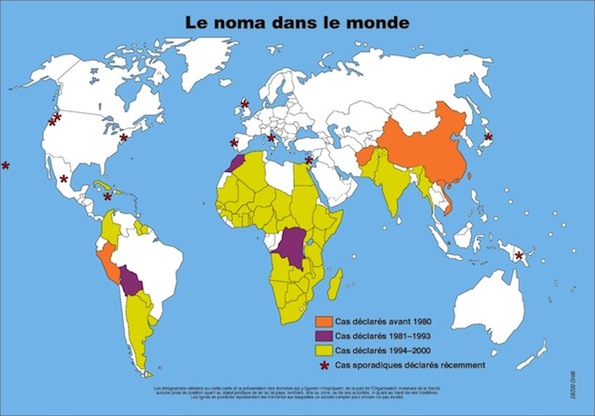 The annual distribution of new cases shows that climatic factors play a role. There is resurgence during the dry season, renamed the “hunger month” by some researchers. Another factor makes it difficult to collect data: most victims will not have time to get to a treatment center before succumbing to the disease. The situation is therefore certainly even more tragic than it appears.
The annual distribution of new cases shows that climatic factors play a role. There is resurgence during the dry season, renamed the “hunger month” by some researchers. Another factor makes it difficult to collect data: most victims will not have time to get to a treatment center before succumbing to the disease. The situation is therefore certainly even more tragic than it appears.
The Winds of Hope Foundation partially funded an epidemiological study of noma in Africa. The study was carried out by the WHO / AFRO and the results, published in 2008, showed that:
• More than 100 000 children are affected by noma every year. The victims are almost all children between the ages of 6 months and 6 years. In the absence of treatment, noma is fatal in 70 to 90% of cases. A reasonable estimate is 80,000 deaths per year.
• 20,000 children per year survive noma, but then live hidden away.
• There are 500,000 noma survivors alive in the world today.
• The poorest countries in Africa, Asia and South America are affected, and Africa is the hardest hit, with 80% of cases.
• Today, noma has become a problem of public health, notably in certain populations of the Sahel region, also designated by some as the "Noma belt".
• Noma and other oral diseases are thought to be on the increase in Africa, due to a general deterioration in living conditions, malnutrition, poor hygiene, HIV / AIDS, conflict, corruption, etc.
• Noma reappears sporadically in developed countries, where its emergence is thought to be related to factors such as HIV / AIDS.
This study is based solely on statistics gathered over 10 years ago by WHO. Further studies are now required.
Geopolitics
Noma is an important public health problem given the seriousness and urgency of the disease. This infectious disease is also an emblematic symbol of extreme poverty, severe malnutrition and social inequities. Appearance of noma is a severe threat to human rights in terms of education, health and food access.
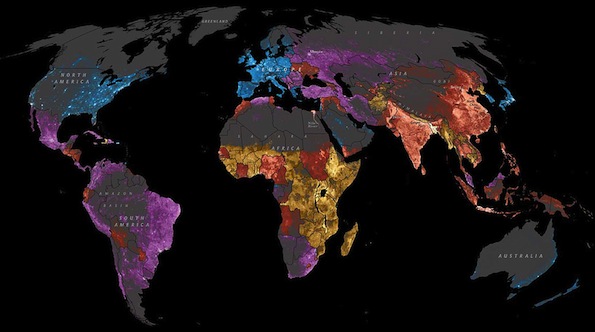
The map shows population density; the brightest points are the highest densities. Each country is colored according to its average annual gross national income per capita using categories established by the World Bank :
• Blue : annual income > 12'000 USD.
• Mauve : annual income ranging between 4'000 and 12'000 USD.
• Red : annual income ranging between 1'000 and 4'000 USD
• Yellow : annual income < to 1'000 USD
Sub-Saharan and Central Africa concentrate the poorest populations in the world which are constantly increasing as a result of climate changes and security issues.
Noma is becoming endemic in many African countries ; Winds of Hope has decided to focus its campaigns in sub-Saharan regions where populations are particularly affected.
It is a struggle against infant mortality, which occurs in less than 8 weeks … As a result of ignorance and the rapid advance of this disease, only 7-8% of children affected by this gangrenous infection reach health facilities in time. All the others, more than 90%, die beforehand....totally ignored by the world.
The disease of Noma lies at the crossroads of problems that are as serious and important as:
• Extreme poverty,
• Malnutrition,
• Oral hygiene,
• Infectious diseases,
• Childhood diseases,
• Ignorance, education,
• Emergency medicine
• Human rights
Because of lack of resources and absence of humanitarian organizations active in the fight against noma, very scarce information exists on the gravity of the situation in Asia and South America.
History
Although known to physicians in Antiquity and described in the Nazi concentration camps, international awareness of the existence of noma was only brought about thanks to the campaigning of Edmond Kaiser.
Noma was known in Ancient times to physcians such as Hippocrates, Gallien, Celsus and Aretaeus of Cappadocia. In Europe, numerous 18th and 19th century texts in France, Germany, Poland, Sweden, the Netherlands, Britain and Spain mentioned this disease. Cases of Noma were also described in the United States in 1826 and 1848. Jules Tourdes of the Strasburg Faculty of Medicine defined noma in his 1848 dissertation "On noma or sphacelus of the mouth in children" as «...a gangrene that starts in the mouth and affects principally children whose general state of health is weakened by poor hygiene and serious childhood illnesses such as the various fevers with rash. The infection starts with a mucous ulcer associated with facial œdema, and then spreads rapidly from inside to outside, destroying soft tissue and bone. It is almost always fatal». In the 20th century, as famine episodes became rare and hygiene more widespread, Noma disappeared from industrialized countries, with the exception of the cases described in Nazi concentration camps in Auschwitz and Belsen.
It was the campaiging of Edmond Kaiser and Yvan Muriset, founders of Sentinelles, that brought to light the fact that noma still existed in some places. It was in 1989 at the General Assembly of the World Health Organization (WHO), that Noma was included for the first time on the international agenda. A major step forward came in 1992, when the WHO adopted a strategy and a plan of action to combat Noma. From that there followed, in 1994, recognition of Noma as a public health issue. An international program for the fight against Noma was implemented, backed by the creation of an international network of action against Noma (RIACN), responsible for monitoring this program.
Faced with inadequate funding - and unfortunately also lack of interest in the international community - the WHO had to scale back its program and relegate responsibility for it to the Regional Office for Africa (WHO/AFRO). Only local campaigns continued to be conducted, using private funds, organized in particular by NGOs Sentinelles, Hilfsaktion, Campaner, Au Fil de la Vie, Hymne aux Enfants and Enfants du Noma. Several surgical missions led by volunteer specialists enabled dozens of children to undergo operations.
It was only in 2000 that the intervention of the Winds of Hope Foundation finally made it possible to re-launch the national programs for the fight against Noma initially planned by the WHO. After a successful experimental phase in Niger, the Foundation signed a five-year partnership agreement with the WHO to extend the campaign to Burkina Faso and Mali, then to Benin, Togo and Senegal.
Studies and Research
Occurrence of noma caused by a sharp decline in immune defenses
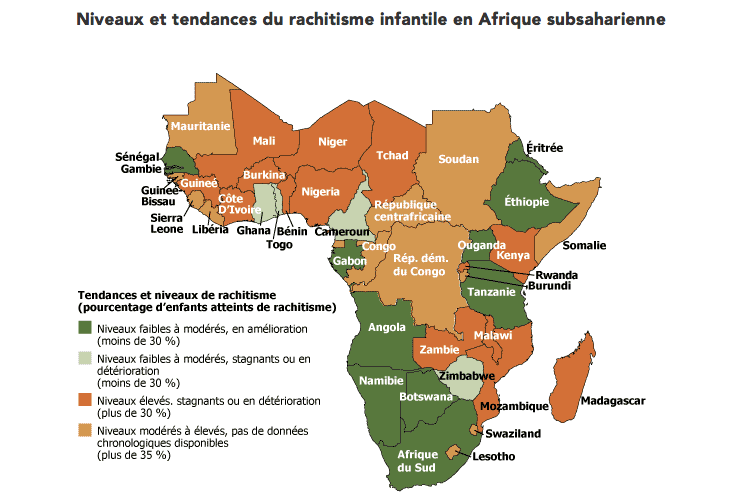
On this map, you can see the incidence of rickets in various regions. The green areas have shown an improvement in child malnutrition rates, while the orange and yellow areas are worse off, with unchanging or worsening rates.
Recent researchs carried out by GESNOMA (Prof. Denis Montandon and Dr. Denise Baratti-Mayer of the University Hospital of Geneva) showed that noma is caused by a sharp decline in the immune defenses, the origin of which is a state of malnutrition and fatigue in the mother during pregnancy, in the presence of a large number of siblings. Doctoral thesis - Dr Denise Baratti Mayer - Étude sur l'étiologie du noma: Aspects microbiologiques et facteurs de risque.
Another etiological research was conducted by GESNOMA in order to define if any bacterial or viral agent could be responsible for this disease. The response was that the appearance of noma is not related to any specfic bacteria or virus. The result of this research was published in the Lancet : Risk factors for noma disease: a 6-years, prospective, matched case-control, study in Niger
source : http://www.prb.org/FrenchContent/2008/StuntingSSAfrica.aspx Charles Teller et al., « Five Emerging Patterns of Demographic, Health and Nutrition Transitions and Stalls in Africa, 1986-2006, » rapport préparé pour l’USAID, août 2007


